AI Virtual Medical Scribe Services: The Future of Clinical Documentation
The Future of Clinical Documentation: Why Healthcare Organizations Are Adopting AI Virtual Scribe Services
For decades, clinical documentation has existed in uneasy tension with clinical care. Physicians trained to practice medicine spend a disproportionate share of their working hours doing something else entirely: documenting it. The problem isn’t new. But the solution, finally, might be.
AI medical scribe technology has moved from experimental novelty to operational infrastructure faster than most healthcare administrators anticipated. The question then is, how must organizations think about adopting it, what it actually delivers, and where the limitations still lie. Let’s explore that in this article.
What AI Medical Virtual Scribes Actually Do
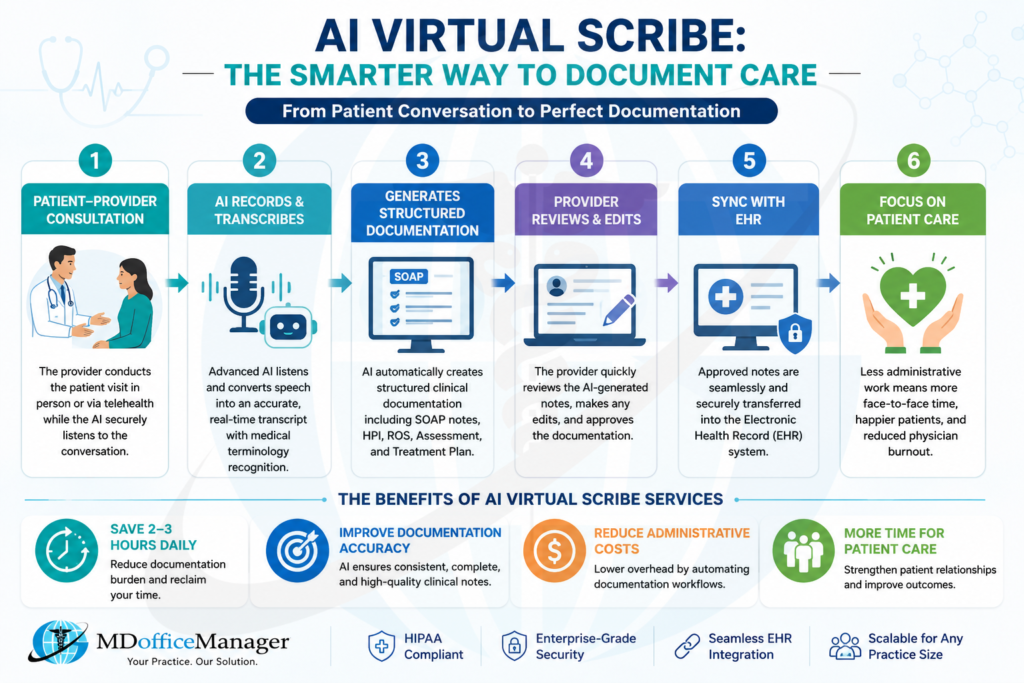
At its core, an AI medical virtually scribe is an ambient listening system. It captures the clinician-patient conversation in real time. Its job is to process natural language using NLP and large language models and produce a structured draft note that the clinician reviews and signs. It’s in either SOAP format, specialty-specific templates, or can be custom configured.
That description makes it sound straightforward. But in practice, the technology is doing several things simultaneously: speaker identification, medical terminology recognition, context inference, and integration with the EHR.
Natural language processing in clinical documentation has evolved considerably from early rule-based systems. Modern platforms combine transformer-based language models with specialty-trained corpora, which is why a cardiology note looks different from a psychiatric intake, the model has learned what each specialty needs.
The ambient paradigm is worth emphasizing. Unlike dictation, the clinician doesn’t press a button or change their behaviour. The system listens passively, which is precisely what makes it lower-friction than prior documentation solutions. Generative AI in healthcare patient summaries has become good enough that the draft output often requires only light editing rather than substantial rewriting.
Why Adoption Is Accelerating
The documented burden is real. Physician burnout surveys have consistently identified administrative documentation as a primary driver of dissatisfaction, and not in a marginal way. Clinicians working in high-volume outpatient settings routinely spend one to two hours per day completing charts after patient encounters, a phenomenon colloquially known as pajama time. This isn’t just a quality-of-life issue; it’s a patient safety and workforce retention concern.
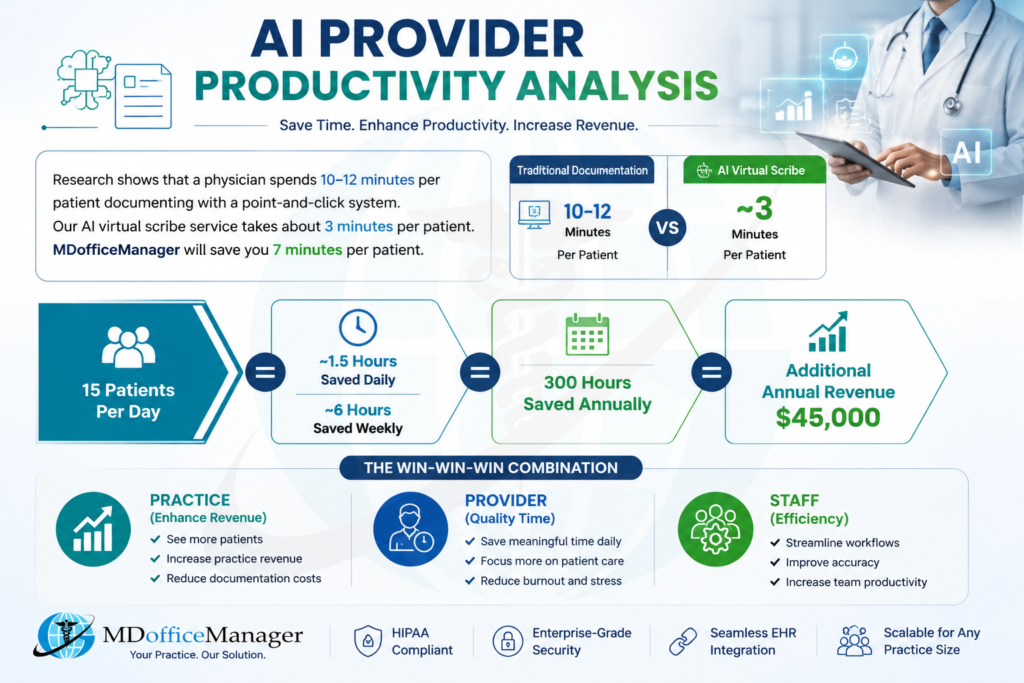
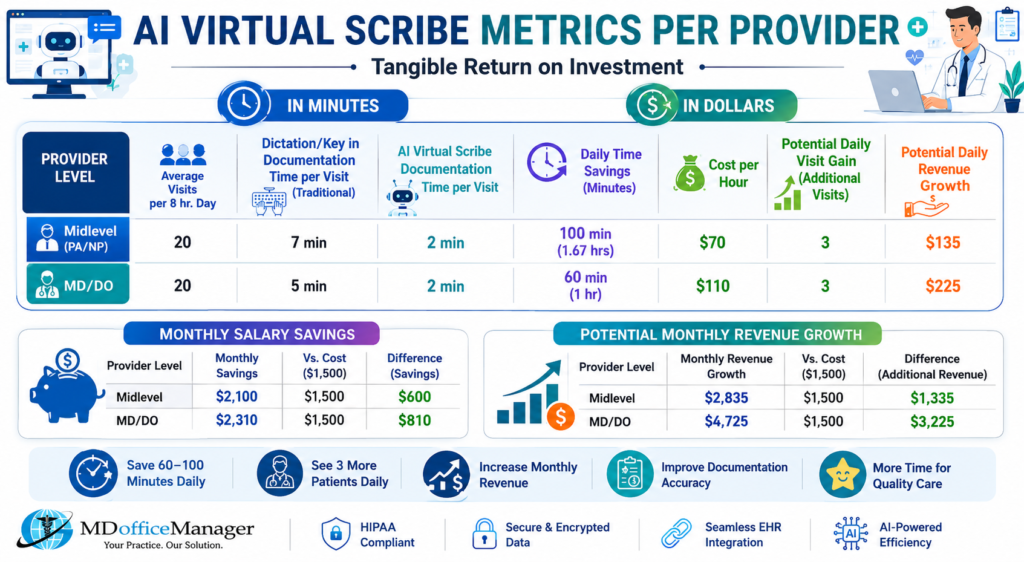
The business case is increasingly quantifiable. Healthcare organizations using AI clinical documentation tools report reductions in documentation time ranging from 20 to 40 percent, with faster chart completion and measurable decreases in after-hours EHR activity. A large 2026 study involving 1,800 clinicians across five academic medical facilities found that AI virtual scribe users saved approximately 90 minutes of documentation time per eight hours of patient care. It’s modest by headline standards, but meaningful when aggregated across hundreds of providers over months.
Equally important is the downstream effect on revenue cycle performance. Incomplete or inconsistently structured AI clinical notes are a primary driver of claim denials; denial rates in many systems hover between 10 and 15 percent of submitted claims. AI-generated documentation, when properly implemented, produces more complete and consistently structured notes that better support medical necessity and coding. That translates directly to reduced denials and improved collections.
The Technology Underneath
It’s worth being precise about the technical architecture, because not all AI medical virtual scribe platforms are equivalent.
The best systems layer multiple capabilities: ambient listening via omnidirectional microphone or device microphone, automated speech recognition tuned for medical vocabulary, NLP-driven entity extraction (diagnoses, medications, vitals, procedures), and generative AI synthesis that assembles extracted entities into a coherent clinical narrative. The final output is mapped to the appropriate documentation structure within the EHR.
HIPAA compliance is non-negotiable. Reputable platforms operate with end-to-end encryption, de-identification protocols, and full audit trail functionality. Any evaluation of an AI clinical documentation vendor should include a thorough review of their BAA, data storage practices, and breach response protocols, not as a formality, but as a clinical governance requirement.
EHR integration depth matters too. A system that generates a note outside the EHR and requires copy-paste adds friction and error risk. Direct integration with platforms like Epic, eClinicalWorks, or Athenahealth, where the draft note populates directly into the patient chart is the standard to hold vendors to.
What a Randomized Controlled Trial Tells Us
The evidence base for AI medical scribe adoption is maturing. A randomized controlled trial published in 2026, involving 304 patients in an adult reconstruction practice, found statistically significant reductions in both physician and administrative processing times with AI scribe use. Critically, there was no significant difference in spelling or grammatical errors between AI-generated and traditionally dictated notes, which addresses a concern frequently raised during early adoption discussions.
What the trial also revealed is that implementation quality matters as much as the technology itself. Clinicians who received structured guidance on how to use ambient AI in healthcare settings showed greater time savings than those who adopted the tool without onboarding support. This is consistent with what experienced health system implementers have learned: AI scribes are not plug-and-play. They require clinical workflow redesign, specialty-specific template tuning, and ongoing quality review.
The Hybrid Model: AI with Human Oversight
A recurring finding in clinical evaluations of AI documentation platforms is that fully automated note generation, without any review layer, introduces error risk that remains unacceptable for final clinical records. Transcription errors do occur.
An AI system may mishear a medication dose, misattribute a symptom, or struggle with overlapping speech in a complex encounter. In one comparative study of commercially available ambient AI scribes, researchers identified errors including misstatement of patient age and inaccurate transcription of medical terminology.
This is why the highest-performing implementations in 2026 operate on a hybrid model: AI-generated documentation combined with professional scribe oversight. The AI delivers speed and scale; the human reviewer provides clinical judgment, coding validation, and error correction before chart finalization. This is not a workaround for inadequate AI, it is a deliberate quality architecture that mirrors how other high-stakes industries have integrated automation with human accountability.
The hybrid model also addresses the liability question that remains front of mind for risk management teams. When a clinician attests to a note, they are responsible for its contents. A model that includes a reviewed, quality-assured draft is one that clinicians can attest to with confidence.
Specialty Considerations
AI clinical documentation does not perform uniformly across specialties, and organizations should approach adoption with that nuance. Structured, procedural encounters like orthopedic follow-ups, straightforward primary care visits, post-operative checks, tend to yield high-quality AI output because the note structure is predictable and the vocabulary is constrained.
Psychiatric encounters present more complexity. Conversation in mental health settings is less structured, more interpersonal, and requires nuanced clinical judgment about what belongs in the record. A simulation-based evaluation of AI scribes in psychiatric consultations found that while documentation efficiency improved, clinicians needed to apply more editorial judgment to AI-generated drafts than in other settings. The technology is improving here, but psychiatrists and behavioral health providers should expect more intensive review workflows during initial implementation.
Similarly, high-acuity emergency settings introduce challenges around multiple simultaneous speakers, ambient noise, and the rapid pace of information exchange during resuscitations or trauma activations. Platforms vary significantly in their robustness to these conditions.
What Healthcare Organizations Should Evaluate
Selecting an AI medical scribe service is a clinical decision as much as a technology procurement decision. The evaluation framework should include:
Documentation quality not just speed. Review sample notes across your most common encounter types. Look for completeness, clinical logic, and accurate capture of assessment and plan.
EHR integration depth. Building direct integration with your existing system is the baseline requirement.
Compliance infrastructure, HIPAA-compliant architecture, BAA availability, audit trails, and data residency commitments.
Oversight model to understand whether the vendor offers any human review layer, or whether the workflow places all quality assurance responsibility on the clinician.
Get implementation support in onboarding, specialty tuning, and ongoing optimization are differentiators that separate good vendor relationships from difficult ones.
The Realistic Outlook
AI medical scribe technology is not a complete solution to clinical administrative burden, and organizations that approach it expecting immediate transformation will be disappointed. The realistic picture is more measured: meaningful time savings, improved documentation consistency, and a better experience for clinicians who engage with the technology seriously. The time savings accrue over weeks and months as clinicians and systems calibrate together.
What the technology does represent, genuinely, is a structural shift in what documentation can look like. The ambient AI in healthcare paradigm is where the conversation itself becomes the source of record, processed in real time and it removes the fundamental friction of the keyboard-and-template model that has governed clinical documentation for thirty years.
As AI continues to reshape healthcare finance, the question is not if organizations should adopt it, but how they can implement it successfully. Achieving meaningful results requires a thoughtful approach that balances efficiency gains, risk management, regulatory compliance, and provider trust.